PUSH Tool 3.0
About the PUSH TOOL
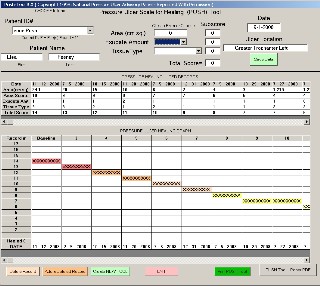
PUSH Screen Shots
PUSH Tool Request Form
Wound-Mapping Information Form
Name*:
Title: (MD, DO, DPM, RN, PT, President, Office Manager, etc)
Address:
Phone:
Email*:
Please Send Information Please Contact Me (Phone Number Please)
PUSH Tool